
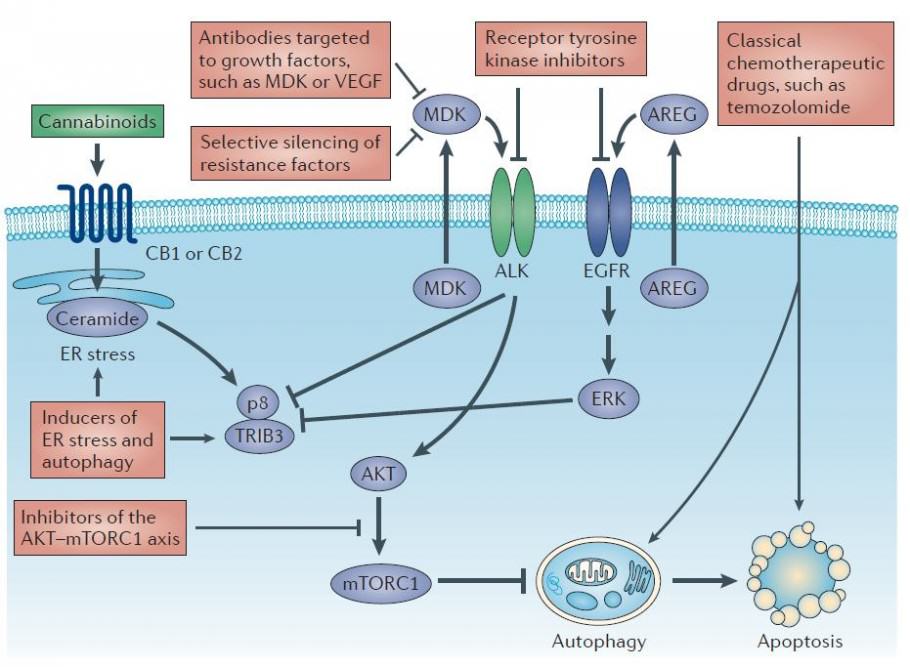
Mechanisms of cannabinoid action against brain tumors
New studies show efficiency of Cannabis against Cancer (2013)
Therefore, we can now find something even more interesting: some cannabinoids in the marijuana plant have a healing action against different forms of cancer.
Several testimonies are available now in social networks, particularly
in the United States, where medical marijuana is much more accessible
than in Europe. Examples of the most common cures are leukemia and brain tumors
(gliomas), usually in children and even babies. However, these numerous
testimonies are not sufficient evidence to convince the medical and
scientific communities, which need reliable studies to confirm these
claims. In order to rectify the situation, we propose here a
(non-exhaustive) list of 68 international scientific publications, drawn from the best research laboratories, demonstrating the efficiency of the cannabinoids found in marijuana plants in the treatment of cancer.
Diagram of the cannabinoid action against cancer cells
Studies on the action of cannabinoids against cancer
- Anti-tumor effects of marijuana. Updated publications on the website of the National Cancer Institute of the Government of the United States in May 2014.
- Preparation and characterisation of biodegradable microparticles filled with THC and their antitumor efficacy on cancer cell lines. Study published in the Journal of Drug Targeting in September 2013.
- The endocannabinoid system: a therapeutic target for regulating the growth of cancer.
- Study published in the Life Science journal in March 2013.
- CBD Cannabidiol as a potential anticancer drug. Study published in the British Journal of Pharmacology in February 2013.
- Cannabinoids as anticancer modulators. Study published in the Progress in Lipid Research journal in January 2013.
- CBD inhibits angiogenesis by multiple mechanisms. Study published in the British Journal of Pharmacology in November 2012.
- Towards the use of cannabinoids as antitumour agents. Study published in Nature in June 2012.
- Cannabinoid-associated cell death mechanisms in tumor models. Study published in the International Journal of Oncology in May 2012.
- Cannabinoids, endocannabinoids and cancer. Study published in Cancer Metastasis Reviews in December 2011.
- The endocannabinoid system and cancer: therapeutic implication. Study published in the British Journal of Pharmacology in July 2011.
-
Marijuana against brain cancer (glioma, glioblastoma…)
- Cannabidiol (CBD), a non-psychoactive cannabinoid compound, inhibits the proliferation and invasion in U87-MG and T98G glioma cells through a multitarget effect. Study published in the Public Library of Science journal in October 2013.
- CBD, a novel therapeutic target against glioblastoma. Study published in Cancer Research in March 2013.
- Local delivery of cannabinoid-filled microparticles inhibits tumor growth in a model of glioblastoma multiforme. Study published in Public Library of Science in January 2013.
- Cannabinoid action inhibits the growth of malignant human glioma U87MG cells. Study published in Oncology Reports in July 2012.
- A combined preclinical therapy of cannabinoids and temozolomide against glioma. Study published in Molecular Cancer Therapeutics in January 2011.
- Cannabidiol enhances the inhibitory effects of THC on human glioblastoma cell proliferation and survival. Study published in the Molecular Cancer Therapeutics journal in January 2010.
- Cannabinoid action induces autophagy-mediated cell death in human glioma cells. Study published in The Journal of Clinical Investigation in May 2009.
- Cannabinoids inhibit glioma cell invasion by down-regulating matrix metalloproteinase-2 expression. Study published in Cancer Research in March 2008.
- Cannabinoids and gliomas, a study published in Molecular Neurobiology in June 2007.
- Cannabinoids inhibit gliomagenesis. Study published in the Journal of Biological Chemistry in March 2007.
- A pilot clinical study of THC in patients with recurrent glioblastoma multiforme. The results were published in the British Journal of Cancer in June 2006.
- Cannabidiol inhibits human glioma cell migration through an independent cannabinoid receptor mechanism. Study published in the British Journal of Pharmacology in April 2005.
- Cannabinoids inhibit the vascular endothelial growth factor pathway (VEGF) in gliomas. Study published in the Journal of Cancer Research in August 2004.
- Antitumor effects of cannabidiol, a nonpsychoactive cannabinoid, on human glioma cell lines. Study published in the Journal of Pharmacology in November 2003.
- Inhibition of glioma growth in vivo by selective activation of the CB2 cannabinoid receptor. Study published in the Journal of Cancer Research in August 2001.
Mechanisms of cannabinoid action against brain tumors
Marijuana against breast cancer
- Targeting multiple cannabinoid antitumor pathways with a resorcinol derivative leads to inhibition of advanced stages of breast cancer. Study published in the British Journal of Pharmacology in June 2014.
- CBDA, an acid form of CBD found in fiber-type cannabis, is an inhibitor of MDA-MB-231 breast cancer cell migration. Study published in Toxicology Letters in November 2012.
- Cannabinoids: A new hope for breast cancer therapy? Study published in Cancer Treatment Reviews in June 2012.
- Pathways mediating the effects of cannabidiol on the reduction of breast cancer cell proliferation, invasion, and metastasis. Study published in Breast Cancer Research and Treatment in August 2011.
- CBD induces programmed cell death in breast cancer cells by coordinating the cross-talk between apoptosis and autophagy. Study published in Molecular Cancer Therapeutics in May 2011.
- Cannabinoids reduce ErbB2-driven breast cancer progression. Study published in Molecular Cancer in July 2010.
- CBD as a novel inhibitor of Id-1 gene expression in aggressive breast cancer cells. Study published in Molecular Therapeutics Research in November 2007.
- Antitumor activity of plant cannabinoids with emphasis on the effect of cannabidiol on human breast carcinoma. Study published in the Journal of the American Society for Pharmacology and Experimental Therapeutics in May 2006.
- THC inhibits cell cycle progression in human breast cancer cells through Cdc2 regulation. Study published in Cancer Research in July 2006.

Explanation of cannabinoid action against breast tumors
Marijuana against blood cancer (leukemia, myeloma, lymphoma…)
- The effects of cannabidiol and its synergism with bortezomib in multiple myeloma cell lines. Study published in the International Journal of Cancer in December 2013.
- Enhancing the activity of CBD and other cannabinoids against leukaemia. Study published in Anticancer Research in October 2013.
- Cannabis extract treatment for terminal acute lymphoblastic leukemia of Philadelphia chromosome (Ph1). Study published in Case Reports in Oncology in September 2013.
- Expression of type 1 and type 2 cannabinoid receptors in lymphoma. Study published in the International Journal of Cancer in June 2008.
- Cannabinoid action in mantle cell lymphoma. Study published in Molecular Pharmacology in November 2006.
- THC-induced apoptosis in Jurkat leukemia. Study published in Molecular Cancer Research in August 2006.
- Targeting CB2 cannabinoid receptors as a novel therapy to treat malignant lymphoblastic disease. Study published in Blood American Society of Hemmatology in July 2002.
Dr William Courtney, Cannabis VS Cancer (2013)
Marijuana against lung cancer
- Cannabinoids increase lung cancer cell lysis by lymphokine-activated killer cells via upregulation of Icam-1. Study published in Biochemical Pharmacology in July 2014.
- Cannabinoids inhibit angiogenic capacities of endothelial cells via release of tissue inhibitor of matrix metalloproteinases-1 from lung cancer cells. Study published in Biochemical Pharmacology in June 2014.
- COX-2 and PPAR-γ confer CBD-induced apoptosis of human lung cancer cells. Study published in Molecular Cancer Therapeutics in January 2013.
- CBD inhibits lung cancer cell invasion and metastasis via intercellular adhesion molecule-1. Study published in the Journal of the Federation of American Societies for Experimental Biology in April 2012.
- Cannabinoid receptors, CB1 and CB2, as novel targets for inhibition of non–small cell lung cancer growth and metastasis. Study published in Cancer Prevention Research in January 2011.
- THC inhibits epithelial growth factor-induced (EGF) lung cancer cell migration in vitro as well as its growth and metastasis in vivo. Study published in the journal Oncogene in July 2007.

Cannabinoids induce apoptosis of various cell types
Cannabinoids against colorectal cancer
- Inhibition of colon carcinogenesis by a standardised Cannabis Sativa extract with high content of CBD. Study published in Phytomedecine in December 2013.
- Chemopreventive effect of the non-psychotropic phytocannabinoid CBD on colon cancer. Study published in the Journal of Molecular Medecine in August 2012.
- Cannabinoids against intestinal inflammation and cancer. Study published in Pharmacology Research in August 2009.
- Action of cannabinoid receptors on colorectal tumor growth. Study published by the Cancer Center of the University of Texas in July 2008.
- Cannabinoid receptor agonist as an alternative drug in 5-Fluorouracil-resistant gastric cancer cells. Study published in Anticancer Research in June 2013.
- Antiproliferative mechanism of a cannabinoid agonist by cell cycle arrest in human gastric cancer cells. Study published in the Journal of Cellular Biochemistry in March 2011.
Marijuana against prostate cancer
- Non-THC cannabinoids inhibit prostate carcinoma growth in vitro and in vivo: pro-apoptotic effects and underlying mechanisms. Study published in the British Journal of Pharmacology in December 2012.
- The role of cannabinoids in prostate cancer: Basic science perspective and potential clinical applications. Study published in the Indian Journal of Urology in January 2012.
- Induction of apoptosis by cannabinoids in prostate and colon cancer cells is phosphatase dependent. Study published in Anticancer Research in November 2011.

Mode of action of cannabinoids against tumor cells
Marijuana against liver cancer
- Involvement of PPARγ in the antitumoral action of cannabinoids on hepatocellular carcinoma (CHC). Study published in Cell Death and Disease in May 2013.
- Evaluation of anti-invasion effect of cannabinoids on human hepatocarcinoma cells. Study published on the site Informa Healthcare in February 2013.
- Antitumoral action of cannabinoids on hepatocellular carcinoma. Study published in Cell Death and Differentiation in April 2011.
Marijuana against pancreatic cancer
- Cannabinoids inhibit energetic metabolism and induce autophagy in pancreatic cancer cells. Study published in Cell Death and Disease in June 2013.
- Cannabinoids Induce apoptosis of pancreatic tumor cells. Study published in Cancer Research in July 2006.
Marijuana against skin cancer
- Cannabinoid receptors as novel targets for the treatment of melanoma. Study published in the Journal of the Federation of American Societies for Experimental Biology in December 2006.
- Inhibition of skin tumor growth and angiogenesis in vivo by activation of cannabinoid receptors. Study published in the Journal of Clinical Investigation, in January 2003.
Cannabis to cure Cancer ? (David Triplett, 2010)
Marijuana against other types of cancer
- Bladder: Marijuana reduces the risk of bladder cancer. Study published in the Medscape site in May 2013.
- Kaposi sarcoma: Cannabidiol inhibits growth and induces programmed cell death in Kaposi sarcoma–associated herpesvirus-infected endothelium. Study published in the journal Genes & Cancer in July 2012.
- Nose, mouth, throat, ear: Cannabinoids like THC inhibit cellular respiration of human oral cancer cells. Study by the Department of Pediatrics at the State University of New York, published in June 2010.
- Bile duct: The dual effects of THC on cholangiocarcinoma cells: anti-invasion activity at low concentration and apoptosis induction at high concentration. Study published in Cancer Investigation in May 2010.
- Ovaries: Cannabinoid receptors as a target for therapy of ovarian cancer. Study published on the American Association for Cancer Research website in 2006.

Efficiency of cannabinoids against cancer
We greatly appreciate the research work carried out by Dr Manuel Guzman’s team at the Universidad Complutense de Madrid for their current work on the use of cannabinoids against cancer.
Do not hesitate to share this information in your community, particularly if you know doctors who do cancer research, and obviously with people suffering from this disease and seeking a natural, effective and safe complementary therapy.
The current legislation on medical marijuana is not adapted to the medical information available today.
http://www.alchimiaweb.com/blogen/68-studies-efficiency-marijuana-against-cancer/








 Before diving into the study, it’s helpful to know that
Before diving into the study, it’s helpful to know that 

